
Curated Information on COVID 19

Welcome to the COVID-19 information page offered by the basic science departments at the University of Michigan. The COVID-19 pandemic has caused a huge disruption in our daily lives and presents a monumental, ongoing public health crisis affecting our community. We recognize that it is difficult to find credible information about COVID-19. Thus, we intend this site as a source of reliable information that is curated by members of our basic science departments with expertise in virology, immunology, epidemiology, genetics, pharmacology, cell biology, biochemistry, informatics, science communication, medicine, and public health. It features new content and links to additional resources that we hope you will find useful.
What is a virus?
An one-hour introduction to “what is a virus,” delivered by Vincent Racaniello, Professor at Columbia University and creator of This Week In Virology podcast.
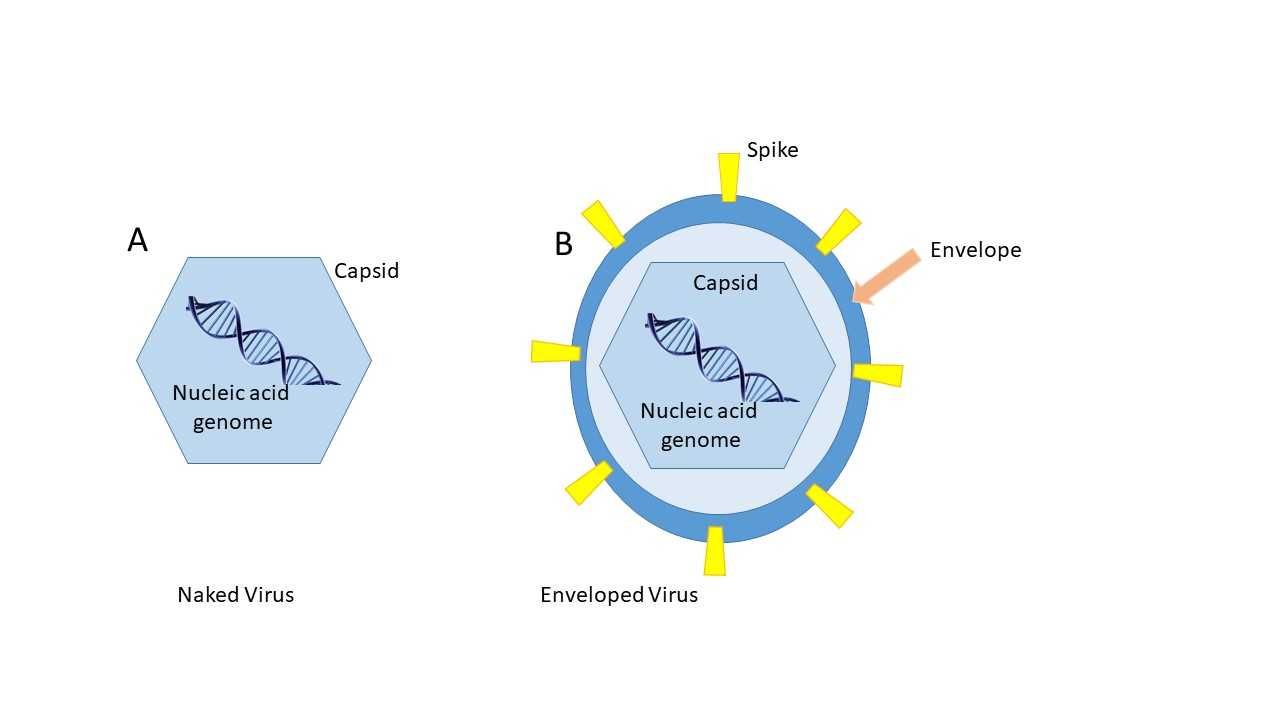
A virus is a sub-microscopic particle consisting of nucleic acid encased in some type of protective shell (the viral capsid) to form the viral genome Viruses with this structure are often called “naked” (panel a). Some viruses also pick up a lipid bilayer of plasma membrane when they replicate in mammalian cells. These viruses are called “enveloped” viruses (panel b). The genomes of viruses can be RNA or DNA and can be single or double-stranded and, in some cases, the virus can have several genome segments. Proteins on the surface of the viral capsid, or that extend through the viral envelope (e.g., spike proteins), are generally the proteins used for attachment to host cells.
{kind=link}
What is COVID-19?

This acronym stands for coronavirus-induced disease identified in 2019. It is caused by infection with the SARS-CoV-2 virus. Many people inaccurately refer to the virus by this name, but COVID-19 is the disease caused by the virus (similar to the concept of AIDS being a disease caused by the HIV virus).
Up to date information regarding confirmed cases, number of people tested, and total deaths broken down by regions around the world is published by the Center for Systems Science and Engineering at Johns Hopkins University:
What is the structure of the SARS-CoV-2 virus?

Source: https://commons.wikimedia.org/wiki/File:3D_medical_animation_corona_virus.jpg
SARS-CoV-2 is a coronavirus of the beta-coronavirus subfamily. It is an enveloped virus with an RNA genome. The spike glycoproteins (which are formed by a trimer of identical molecules) are embedded in the viral envelope and appear “crown-like” when viewed under a microscope and this is where the name comes from. The spike glycoprotein is the molecule the virus uses to bind to mammalian cells.
What is the receptor for SARS-CoV-2 in humans?
Thus far, the only receptor identified is the angiotensin converting enzyme (ACE-2) receptor. The ACE-2 receptor is an enzyme on the surface of cells in the lung, blood vessels, kidney, and intestines. The normal function of the receptor is to catalyze the conversion of angiotensin II to angiotensin (1-7). In this way ACE-2 normally works to lower blood pressure. In order for the viral envelope to fuse with the host membrane to deliver its genome during viral entry, the S protein of the virus must undergo a proteolytic cleavage event. This cleavage is mediated by TMPRSS2, which is a transmembrane protease enzyme. Michigan’s own Arul Chinnaiyan is looking into the possibility of blocking this enzyme as a treatment. It is possible there are other receptors for the virus that may participate as well. CD13 is a potential receptor being investigated by Michigan investigator, David Fox. Other related coronaviruses use a number of different cell surface molecules as receptors. Middle East respiratory syndrome (MERS) coronavirus binds to dipeptidyl peptidase 4 (DPP4; also known as CD26); Murine hepatitis virus (MHV) binds carcinoembryonic antigen-related cell adhesion molecule 1 (CEACAM1), and transmissible gastroenteritis virus (TGEV) binds to aminopeptidase N.
{kind=link}
How did the pandemic start?
SARS-CoV-2 was likely circulating in bats before infecting a person. This form of transmission is known as a zoonosis (from animal to human transmission). While widely reported that the virus originated in a person working in a food market in Wuhan, China, sparking a cluster of infections reported on Dec. 21, 2019, new evidence suggests the first case may have happened around Dec. 1st in an individual with no known connection to the Wuhan market. Once the virus transmitted to humans, it was readily spread person to person via respiratory secretions. An excellent resource discussing the origin and emergence of SARS-CoV-2 (including genomic diversity) can be found here. This same resource highlights that mutation of the viral genome seen via sequencing is not necessarily an indication that these mutations will lead to radical changes in transmissibility, or virulence.
This article highlights that there is no credible evidence to support the claims of laboratory engineering of SARS-CoV-2: Please click here.
Transmission of SARS-CoV-2
U of M Grand Rounds by Dr. Joel Howell - 04/17/20
The virus is believed to be transmitted in large droplets (5-10 µM) in size that are large enough that they fall to the ground quickly. Thus, the virus is thought to be transmitted by coughing or sneezing when people are within 1 meter (~3 feet) of each other. This is the reason for the recommended 6 feet of distance between people under current social distancing guidelines. Transmission can also occur if you touch a contaminated object (known as a fomite) that has been contaminated by a virus-containing respiratory droplet. This is the reason for the recommended hand hygiene (washing hands often or using alcohol based sanitizer with >60% alcohol content). Airborne transmission (as occurs with the much more contagious measles virus) is the spread by small droplets (<5 µM) that stay suspended in air for long periods of time such that someone walking through a room where an infected person has been is more likely to breathe in a contaminated small droplet. Under certain conditions that generate aerosols (e.g. ventilation in hospitalized patients), it is possible that SARS-CoV-2 could be transmitted by aerosolized small droplets. This is the reason for health care workers in high risk settings to use specialized N-95 masks that limit inhalation of small droplets. There is some evidence that SARS-CoV-2 can replicate in the GI tract and viral RNA can be found in feces, but live virus has only been cultured in a single specimen thus far. Under certain conditions that generate aerosols (e.g. ventilation in hospitalized patients), it is possible that SARS-CoV-2 could be transmitted by aerosolized small droplets. This is the reason for health care workers in high risk settings to use specialized N-95 masks which limit inhalation of small droplets.

SARS-CoV-2 Release from Infected Cells Credit: Rocky Mountain Laboratories, National Institute of Allergy and Infectious Diseases, Hamilton, MT
It is clear that handwashing is a major deterrent to spreading disease. Dr. Joel Howell recently gave a Grand Rounds lecture on the history of Ignaz Semmelweis and the discovery that this saved lives! See link below.
How does SARS-CoV-2 cause disease?
SARS-CoV-2 is a lytic virus, which means that during replication in the lung, it can cause destruction of cells within the respiratory tract. Recognition of the virus by innate immune cells can lead to production of pro-inflammatory cytokines and chemokines which have the capacity to cause fever, inflammation, and, in cases of severe disease, vascular and epithelial barrier dysfunction leading to flooding of the alveoli in the lungs (pneumonia), making it hard to breathe and limiting the ability of the lungs to take in oxygen and diffuse carbon dioxide. One early study of 41 patients suggested common symptoms were fever (98%), cough (76%), myalgia or fatigue (44%), and atypical symptoms included sputum (28%), headache (8%), hemoptysis (coughing up blood) (5%), and diarrhea (3%). Nearly half of the patients had difficulty breathing, with most exhibiting this complication about 8 days after first symptoms. Sixty-three percent (63%) of patients showed a reduction in their peripheral blood lymphocyte counts, which could impact the ability of the adaptive immune response to clear the virus. Complications included acute respiratory distress syndrome (29%), acute heart injury (12%), and secondary infections (10%); Thirty-two percent (32%) of the patients required ICU-level care. [Source: The Lancet. 2020; 395: 497-506]. An epidemiological study in China demonstrated evidence of asymptomatic infection in some people as well (~1.2% of patients in this study) [Chinese Journal of Epidemiology. 2020; 41: 145-151]
NOTE THIS NEW INFO AS OF today 4-17-20:
The CDC has updated its list of symptoms of COVID-19. The full list now includes: fever, cough, shortness of breath/difficulty breathing, chills, repeated shaking with chills, muscle pain, headache, sore throat, new loss of taste or smell.
KQED, a Bay Area PBS station has created a very short and informative video about how SARS-CoV-2 attacks the lungs. See the 5 minute Deep Look episode here:
In this Nature Reviews Microbiology article,Thiel and colleagues discuss the key aspects of coronavirus biology and their implications regarding infection, treatment and prevention: https://www.nature.com/articles/s41579-020-00468-6
Health Disparities and COVID-19
Dr. Oveta Fuller, Associate Professor of Microbiology and Immunology and ordained minister was interviewed on the webinar: Michigan Black Caucus of Local Elected Officials COVID-19 Discussion on April 14, 2020. Content includes a lay summary of virus origin, transmission, biology of coronavirus respiratory disease and why available preventions work. It also covers discussion of how this pandemic has hit the African American community especially hard and explores some of the reasons such as underlying co-morbidities, medical care access and overrepresentation in essential jobs that put this community at greater infection risk.
What are limitations to ramping up COVID-19 testing at UM now?

This image shows an NP swab collection for COVID-19 testing described in this NEJM article: https://www.nejm.org/doi/full/10.1056/NEJMvcm2010260
The clinical microbiology lab has to operate under CLIA certified rules and regulations…which dictate what type of machine can be used, what controls are used, training for the personnel and how often they are inspected, etc. The limit in testing for virus currently is the ability of the supply chain to meet demand of the viral transport media and the testing swabs for weeks to come…causing them to limit usage now. Pharmacy is now helping to make the viral transport media. The testing swabs are quite unique. Apparently they are truly an engineering marvel. They are plastic and flexible and THIN to allow to reach from the nasal cavity all the way back to the nasopharynx to get a good sample (see image below). They are flocked in such a way that they capture sample and then release it when it hits liquid so that they can extract the sample for PCR. Regular Q-tips with wooden shafts can break off while collecting sample in people’s noses. They also have cotton fibers that shed and inhibit the PCR reactions. Using an oropharyngeal swab is less sensitive, although easier to get. Regarding the serology tests, there are a lot of potential issues there as well, including sensitivity and specificity…especially when most of the population should be negative. Even if the test has a small error rate, when lots of people are getting tested, that could mean a lot of false positives or negatives.
A very accessible NPR article about the potential problems with antibody testing can be read or heard here.
Also, a UM article regarding considerations for antibody testing before returning to work at UM can be found here.
A lay summary regarding the possibility of saliva testing is found here.
Treatments for COVID-19
Currently, there are no established treatments for SARS-CoV-2. The University of Michigan Office of Research is maintaining a database to provide an up-to-date list of COVID-19 research findings (publications, data sets, and clinical trials) in a single place, without requiring any special access permissions or complex queries. The sheet contains a tab for each type of output and can be accessed at this link. It will continue to be updated daily for the foreseeable future. Please click here to see dimensions COVID-19 publications, data sets, clinical trials.
Here at Michigan, the following trials are actively enrolling patients:
Sarilumab for Hospitalized Patients (PI: Gregg) Sarilumab (Kevzara) — jointly developed Regeneron and Sanofi — is a fully human, monoclonal antibody that inhibits the interleukin-6 (IL-6) pathway by binding and blocking the IL-6 receptor. If you want to see a short article about how the cytokine storm promotes the pathogenesis of COVID-19, please click here.
Remdesivir for Moderately Ill Patients (PI: Kaul) Remdesivir is an anti-viral medication developed by Gilead Sciences. It is an adenosine analogue which inserts into viral RNA chains, potentially causing premature termination. It was initially developed as a treatment for Hepatitis C, Ebola, and Marburg virus infections. Information about a trial in monkeys conducted by the NIAID can be found here.
If you are interested in the chemistry of Remdesivir, here is a nice interactive article that explains it.
The following link is an up to date tracker for the COVID clinical trials that are open, completed or not yet active at Michigan: https://docs.google.com/spreadsheets/d/1nAQ8K1pKG1YQGQJCGbPkoOCMVc53INnI...
Neurological and Psychiatric impact of COVID-19
While respiratory failure associated with COVID-19 has received most of the attention, this disease also disrupts the function of the nervous system at many levels. Initially, during the early phases of infection the immune response causes an increase in the level of cytokines that can mediate the headaches associated with the disease (Lancet 2020; 395: 497 and The Journal of Headache and Pain 2020; 21:38). Rare reports of acute necrotizing encephalopathy and encephalitis associated with COVID-19 may also be mediated by the so-called “cytokine storm.” and Brain Beh Immun Patients with COVID-19 may also experience an increase in blood clots, which increases the risk for stroke caused by blood clots in the brain (The New England Journal of Medicine. 10.1056/NEJMc2009787). The longer-term effects of COVID-19 are uncertain, but the SARS-CoV-2 coronavirus is a member of the betacoronavirus genus which also includes the SARS-CoV-1 and MERS-CoV viruses. A significant concern for the neuroscience community is that like SARS-CoV-1, the SARS-CoV-2 may spread either transsynaptically or by crossing the blood-brain barrier to infect neurons and glia of the central nervous system to produce long-lasting effects following infection of COVID-19 patients. Read more here. This will certainly be an area of active research for the future.
COVID-19 illness triggers a perfect storm of events that will leave survivors and their loved ones at high risk for symptoms of depression, anxiety, and post-traumatic stress disorder (JAMA Intern Med. Doi:10.1001/jamainternmed.2020.1562). These include the experience of social isolation during illness and quarantine, traumatic memories from the time in the hospital such as feeling unable to breathe or pain from medical procedures, and the long-lasting impact of inflammation and the hormonal stress response in the brain itself. At the Michigan Neuroscience Institute many of our faculty are working hard in and out of the laboratory to understand the impact of this disease on the brain and behavior.
A short opinion piece about how loss of smell and taste hint about effects of COVID-19 in the nervous system can be found here.
SARS-CoV-2 Genetic Variants
There has been significant concern over the identification of news variants of SARS-CoV-2 that are more transmissible. The Science paper describing this can be found here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7775736/
Thus far, the variants that have been detected are still effectively managed by available vaccine strategies. Dr. Adam Lauring gave a nice interview with JAMA regarding SARS-CoV-2 Genetic Variants that can be heard here:
https://html5-player.libsyn.com/embed/episode/id/17385050/theme/custom/height/480/width/640/menu/no